epidemics is an R package that provides modular representations of populations and public health response measures, allowing them to be combined with epidemiological model structures curated from the published literature, to conveniently compose and compare epidemic scenario models.
The models in epidemics focus on directly transmitted infections, and implement methods outlined in Bjørnstad et al. (2020a) and Bjørnstad et al. (2020b). The models in epidemics can help provide rough estimates of the course of epidemics, and the effectiveness of pharmaceutical and non-pharmaceutical interventions.
epidemics relies on Eigen via {RcppEigen}, and on Boost Odeint via {BH}, and is developed at the Centre for the Mathematical Modelling of Infectious Diseases at the London School of Hygiene and Tropical Medicine as part of the Epiverse-TRACE initiative.
Installation
The current development version of epidemics can be installed from GitHub using the pak package.
if(!require("pak")) install.packages("pak")
pak::pkg_install("epiverse-trace/epidemics")Alternatively, install pre-compiled binaries from the Epiverse TRACE R-universe
install.packages("epidemics", repos = c("https://epiverse-trace.r-universe.dev", "https://cloud.r-project.org"))Installation Notes
Some users who are also using or developing packages that use Stan might face issues if they have modified their toolchain to accommodate packages such as cmdstanr; see this resolved issue for a starting point if you face similar problems.
Users on Windows systems will need to have packages from the RTools family installed and on their system path; see this link for guidance on using RTools for your version of R.
The examples in this README and in the package vignettes build a social contact matrix from demography data in wpp2024, which is not on CRAN and so is not installed alongside the other suggested packages; install it with
pak::pkg_install("PPgp/wpp2024"). You only need it to run the documentation examples, as epidemics itself does not use wpp2024 at runtime.
Quick start
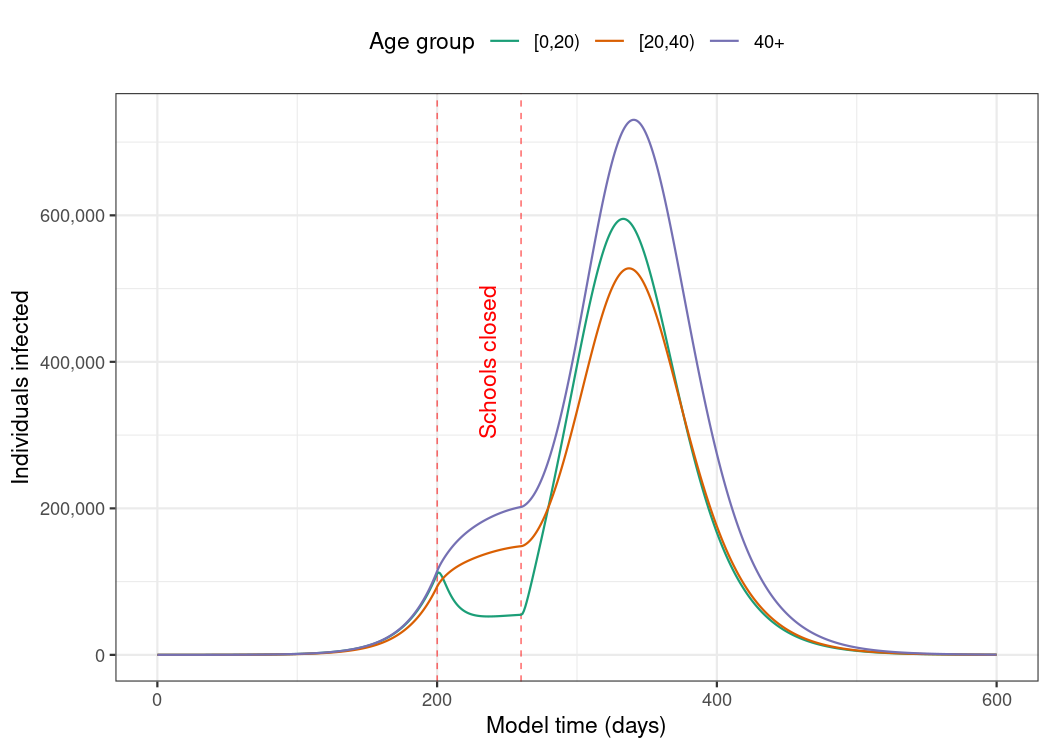
Here we show an example of using the default model in epidemics to model an epidemic in the U.K. population with an similar to that of pandemic influenza, with heterogeneity in social contacts among different age groups, and with the implementation of school closures to dampen the spread of the infection.
Prepare the social contact pattern for a population (here, the U.K population), divided into three age groups: 0 – 19, 20 – 39, and 40+.
# load contact and population data from socialmixr::polymod
polymod <- socialmixr::polymod
# demography data from the wpp2024 package
data("popAge1dt", package = "wpp2024")
uk_pop <- popAge1dt |>
dplyr::filter(name == "United Kingdom", year == 2006) |>
dplyr::select(lower.age.limit = age, population = pop) |>
dplyr::mutate(population = population * 1000)
contact_data <- socialmixr::contact_matrix(
polymod,
countries = "United Kingdom",
survey_pop = uk_pop,
age_limits = c(0, 20, 40),
symmetric = TRUE,
return_demography = TRUE
)
# prepare contact matrix
contact_matrix <- contact_data[["matrix"]]
# prepare the demography vector
demography_vector <- contact_data[["demography"]][["population"]]
names(demography_vector) <- colnames(contact_matrix)Prepare the initial conditions for the population by age group — here, one in every million individuals is infected at the start of the epidemic (for a total of about 60 infections).
# initial conditions: one in every 1 million is infected
initial_i <- 1e-6
initial_conditions <- c(
S = 1 - initial_i, E = 0, I = initial_i, R = 0, V = 0
)
# build for all age groups
initial_conditions <- rbind(
initial_conditions,
initial_conditions,
initial_conditions
)
rownames(initial_conditions) <- colnames(contact_matrix)Prepare an object of the class <population>, using the function population().
# prepare the population to model as affected by the epidemic
uk_population <- population(
name = "UK",
contact_matrix = contact_matrix,
demography_vector = demography_vector,
initial_conditions = initial_conditions
)Define an intervention to close schools for two months. This intervention mostly only affects individuals in the age range 0 – 19, and reduces their contacts by 50%, reducing the contacts of other age groups by 1%. This is an object of the class <contacts_intervention>, created using the function intervention(), while setting type = "contacts".
# an intervention to close schools
close_schools <- intervention(
type = "contacts",
time_begin = 200,
time_end = 260,
reduction = matrix(c(0.5, 0.01, 0.01))
)
# view the intervention
close_schools
#>
#> Intervention name:
#>
#> Begins at:
#> [1] 200
#>
#> Ends at:
#> [1] 260
#>
#> Reduction:
#> Interv. 1
#> Demo. grp. 1 0.50
#> Demo. grp. 2 0.01
#> Demo. grp. 3 0.01Run the default epidemic model, using the function model_default(). We assume an of 1.5 which is similar to pandemic influenza, an infectious period of 7 days, and a pre-infectious period of 3 days. From these values we can calculate transmission rate 1.5 / 7.0, infectiousness_rate 1.0 / 3.0 and recovery_rate 1.0 / 7.0.
# run an epidemic model using `epidemic()`
output <- model_default(
population = uk_population,
transmission_rate = 1.5 / 7.0,
infectiousness_rate = 1.0 / 3.0,
recovery_rate = 1.0 / 7.0,
intervention = list(contacts = close_schools),
time_end = 600, increment = 1.0
)Visualise the development of individuals in the “infectious” compartment over model time. Note that these curves represent the number of individuals that are infectious, and not the number of newly infectious individuals.
Package vignettes
More details on how to use epidemics can be found in the online documentation as package vignettes.
Package models
epidemics provides a convenient interface to a library of compartmental models that can help to model epidemic scenarios for directly transmitted respiratory infections such as influenza or Covid-19 as well haemorrhagic fevers such as Ebola virus disease:
A deterministic SEIR-V model with susceptible, exposed, infectious, recovered, and vaccinated compartments (SEIR-V), allowing for heterogeneity in social contacts, the implementation of a group-specific non-pharmaceutical intervention that reduces social contacts, and a vaccination regime with group-specific start and end dates;
The deterministic Vacamole model developed at RIVM, the Dutch Public Health Institute for the Covid-19 pandemic, with a focus on scenario modelling for hospitalisation and vaccination (Ainslie et al. 2022);
A stochastic, discrete-time, compartmental SEIR model suitable for modelling haemorrhagic fevers such as Ebola Virus Disease, including hospitalisation and hospital and funeral transmissions, adapted from Li et al. (2019) and Getz and Dougherty (2018);
An initial implementation of a compartmental model for diphtheria in the context of internally displaced persons camps, including a reporting rate, hospitalisation rate, and delays in entering and leaving hospital, taken from Finger et al. (2019).
More models are planned to be added in the near future. Please get in touch if you would like to see your model added to the epidemics model library — we are happy to help with translating it into our framework, with a special focus on making the model applicable to LMIC settings.
Related projects
epidemics aims to be a library of published epidemiological models, and the following projects may be useful for building your own models:
- The R package finalsize is also developed by Epiverse-TRACE and helps to calculate the final size of an epidemic in a heterogeneous population, and is a quicker option for estimates of total infections when the temporal dynamics are less important;
- The Epirecipes project is a cookbook-style guide that focuses on different ways to implement epidemic models in R and other languages;
- The R package odin generates systems of ordinary differential equations (ODE) and integrate them, using a domain specific language (DSL), and is widely used to translate compartmental models from R to C code for performance gains;
- Many R packages provide modelling options, and these can be found on the CRAN Epidemiology Task View under the section “Infectious disease modelling”.
Help
To report a bug please open an issue.
Contribute
Contributions to epidemics are welcomed via pull requests.
Code of conduct
Please note that the epidemics project is released with a Contributor Code of Conduct. By contributing to this project, you agree to abide by its terms.